Журнал «Здоровье ребенка» Том 20, №2, 2025
Вернуться к номеру
Етіологічна характеристика та чутливість до антибіотиків збудників гнійно-запальних захворювань щелепно-лицевої ділянки
Авторы: Шевчук В.А. (1), Одушкіна Н.В. (1), Ткаченко М.В. (1), Коваленко Н.І. (1), Смородський В.О. (1), Ткаченко І.Г. (1), Соловйова А.Г. (2)
(1) - Харківський національний медичний університет, м. Харків, Україна
(2) - Харківська обласна дитяча клінічна лікарня, м. Харків, Україна
Рубрики: Педиатрия/Неонатология
Разделы: Клинические исследования
Версия для печати
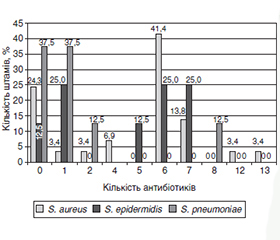
Актуальність. Глобальною проблемою є швидке поширення антибіотикорезистентних збудників інфекційних захворювань. Мета: визначення чутливості до антибіотиків збудників гнійно-запальних захворювань щелепно-лицевої ділянки. Матеріали та методи. Проведено ретроспективне дослідження з використанням медичної документації 59 дітей віком від 2 місяців до 17 років. Аналізували результати мікробіологічного дослідження виділень з рани та визначення чутливості бактерій до антибіотиків. Результати. Із 62 ізольованих штамів бактерій найчастіше виділялися S. aureus (46,8 %), S. epidermidis і S. pneumoniae (по 12,9 %). Інші бактерії (E. faecalis, S. viridans, P. diminuta, Lactobacillus spp., Prevotella spр. і Peptostreptococcus spp.) виявлялися менше ніж у 10 % випадків. Бактерії були у монокульурі і в двокомпонентних асоціаціях. Усі досліджені штами S. aureus, S. epidermidis, S. pneumoniae проявили чутливість до захищених пеніцилінів, оксациліну, цефепіму, цефтароліну, цефтобіпролу, карбапенемів, рифампіцину, оксазолідинонів. Стафілококи також були чутливі до цефазоліну, цефадроксилу, цефалексину, цефаклору, аміноглікозидів, тайгецикліну, моксифлоксацину. Найбільшу стійкість стафілококи мали до бензилпеніциліну, ампіциліну, тикарциліну, піперациліну (68–80 %), пневмокок — до норфлоксацину (80 %). S. aureus був резистентним до макролідів, тетрациклінів, норфлоксацину, хлорамфеніколу. S. epidermidis виявився стійким до макролідів, цефуроксиму, цефтріаксону та цефотаксиму. Пневмокок характеризувався стійкістю до макролідів, тетрациклінів та ампіциліну. Кількість резистентних штамів S. epidermidis становила 87,5 %, S. aureus — 75,7 %, S. pneumoniae — 62,5 %. Кількість антибіотиків, до яких був стійкий S. aureus, коливалася від шести до тринадцяти, S. epidermidis — від одного до семи препаратів, S. pneumoniae — від одного до восьми антибіотиків. Висновки. Серед збудників гнійно-запальних захворювань щелепно-лицевої ділянки переважають грампозитивні факультативно-анаеробні бактерії, насамперед S. aureus, S. epidermidis і S. pneumoniae, які мають множинну резистентність до антибіотиків.
Background. The rapid spread of antibiotic-resistant pathogens of infectious diseases is a global problem. The purpose of this study was to determine antibiotic sensitivity of causative agents of purulent-inflammatory diseases of the maxillofacial region. Materials and methods. The medical records of 59 patients aged from 2 months to 17 years were examined retrospectively. The results of microbiological examination of wound discharge and sensitivity of bacteria to antibiotics were analyzed. Results. Sixty-two isolated bacterial strains were identified, mainly S.aureus (46.8 %), S.еpidermidis (12.9 %) and S.pneumoniae (12.9 %). Other bacteria (E.faecalis, S.viridans, P.diminuta, Lactobacillus spp., Prevotella spp. and Peptostreptococcus spp.) were detected in less than 10 % of cases. All strains of S.aureus, S.epidermidis, S.pneumoniae exhibited sensitivity to penicillinase-resistant penicillins, oxacillin, cefepime, ceftaroline, ceftobiprole, carbapenems, rifampicin, oxazolidinones. Staphylococci were also sensitive to cefazolin, cefadroxil, cephalexin, cefaclor, aminoglycosides, tigecycline, moxifloxacin. Staphylococcus had the superresistance to benzylpenicillin, ampicillin, ticarcillin, piperacillin (68–80 %), pneumococcus — to norfloxacin (80 %). S.aureus was resistant to macrolides, tetracyclines, chloramphenicol. S.epidermidis was resistant to macrolides, cefuroxime, ceftriaxone, and cefotaxime. Pneumococcus exhibited resistance to macrolides, tetracyclines and ampicillin. The amount of resistant strains of S.epidermidis, S.aureus and S.pneumoniae was 87.5, 75.7, and 62.5 %, respectively. The number of antibiotics to which S.aureus was resistant ranged from 6 to 13, S.epidermidis — from 1 to 7, and S.pneumoniae — from 1 to 8. Conclusions. Among the pathogens of purulent-inflammatory diseases of the maxillofacial region, gram-positive facultative anaerobic bacteria predominate, primarily S.aureus, S.epidermidis, and S.pneumoniae, which have multiple resistance to antibiotics.
щелепно-лицева ділянка; гнійно-запальні захворювання; етіологія; антибіотикорезистентність збудників; діти
maxillofacial region; purulent-inflammatory diseases; etiology; antibiotic resistance of pathogens; children
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Mahmudov Jahongirmirzo Komilovich. Purulent-Inflammatory Diseases of the Maxillofacial Region in Patients with Various Chronic Di–seases. Indonesian Journal of Innovation Studies. 2022;18. https://doi.org/10.21070/ijins.v18i.637.
- Steblovskyi D, Skikevich M, Bondarenko V. Structural features of purulent inflammatory diseases of the maxillofacial region in residents of the Poltava region. Ukrainian Dental Almanac. 2020;4:50-52. https://doi.org/10.31718/2409-0255.4.2020.09.
- Wang Z, Sun W, Yang X, et al. Clinical analysis of patients with oral and maxillofacial infections in oral emergency. Beijing Da Xue Xue Bao Yi Xue Ban. 2023 Jun 18;55(3):543-547. doi: 10.19723/j.issn.1671-167X.2023.03.022. (in Chinese).
- Fu XJ, Li WS, Xiang L, Liao LS. Analysis of 256 pediatric oral and maxillofacial emergency in-patients during the outbreak of –COVID-19. Dent Traumatol. 2022 Oct;38(5):367-373. doi: 10.1111/edt.12759.
- Weise H, Naros A, Weise C, et al. Severe odontogenic infections with septic progress — a constant and increasing challenge: a retrospective analysis. BMC Oral Health. 2019 Aug 2;19(1):173. doi: 10.1186/s12903-019-0866-6.
- Bougatef H, Moussaoui E, Kallel I, et al. Periostitis Ossificans: Report of Two Cases Resolved with Endodontic Treatment. Case Rep Dent. 2020 Nov 24;2020:8876268. doi: 10.1155/2020/8876268.
- Rajendra Santosh AB, Ogle OE, Williams D, Woodbine EF. Epidemiology of Oral and Maxillofacial InfectionS. Dent Clin North Am. 2017 Apr;61(2):217-233. doi: 10.1016/j.cden.2016.11.003.
- Vardas E, Adamo D, Canfora F, et al. Impact of COVID-19 Disease on the Development of Osteomyelitis of Jaws: A Systematic Review. J Clin Med. 2024 Jul 23;13(15):4290. doi: 10.3390/jcm13154290.
- Yang W, Hu L, Wang Z, et al. Deep Neck Infection: A Review of 130 Cases in Southern China. Medicine (Baltimore). 2015 Jul;94(27):e994. doi: 10.1097/MD.0000000000000994.
- Gualtero DF, Lafaurie GI, Buitrago DM, et al. Oral microbiome mediated inflammation, a potential inductor of vascular diseases: a comprehensive review. Front Cardiovasc Med. 2023 Aug 30;10:1250263. doi: 10.3389/fcvm.2023.1250263.
- Teal L, Sheller B, Susarla HK. Pediatric Odontogenic Infections. Oral Maxillofac Surg Clin North Am. 2024 Aug;36(3):391-399. doi: 10.1016/j.coms.2024.03.005.
- Peng X, Cheng L, You Y, et al. Oral microbiota in human syste–matic diseases. Int J Oral Sci. 2022 Mar 2;14(1):14. doi: 10.1038/s41368-022-00163-7.
- Khmiz T, Tkachenko M, Kovalenko N, et al. Importance of antimicrobial factors for microbiocenosis and local immunity of the oral cavity in children with mucoviscidosis. Pol Merkur Lekarski. 2022 Jun 24;50(297):190-194. PMID:35801603.
- Rasteniene R, Simenaite G, Brukiene V. Maxillofacial infections in lithuanian hospitalised children and adolescents: a 17-years retrospective study. Eur Arch Paediatr Dent. 2023 Oct;24(5):603-611. doi: 10.1007/s40368-023-00824-z.
- Rastenienė R, Pūrienė A, Aleksejūnienė J, et al. Odontoge–nic Maxillofacial Infections: A Ten-Year Retrospective Analysis. Surg Infect (Larchmt). 2015 Jun;16(3):305-12. doi: 10.1089/sur.2013.264.
- Zhou J, Wan T, Miao R, et al. Oral and maxillofacial emergencies: A retrospective study of 5220 cases in West China. Dent Traumatol. 2023 Apr;39(2):140-146. doi: 10.1111/edt.12798.
- Samaranayake L, Matsubara VH. Normal oral flora and the oral ecosystem. Dent Clin North Am. 2017;61:199-215. https://doi.org/10.1016/j.cden.2016.11.002.
- Tan FY, Selvaraju K, Audimulam H, et al. Length of hospital stay among oral and maxillofacial patients: a retrospective study. J Korean Assoc Oral Maxillofac Surg. 2021 Feb 28;47(1):25-33. doi: 10.5125/jkaoms.2021.47.1.25.
- Tang KWK, Millar BC, Moore JE. Antimicrobial Resistance (AMR). Br J Biomed Sci. 2023;80:11387. doi: 10.3389/bjbs.2023.11387.
- Umeshappa H, Shetty A, Kavatagi K, et al. Microbiological profile of aerobic and anaerobic bacteria and its clinical significance in antibiotic sensitivity of odontogenic space infection: A prospective study of 5 years. Natl J Maxillofac Surg. 2021 Sep-Dec;12(3):372-379. doi: 10.4103/njms.NJMS_1_20.
- Judith MJ, Aswath N, Padmavathy K. Microbiota of Dental Abscess and their Susceptibility to Empirical Antibiotic Therapy. Contemp Clin Dent. 2022 Oct-Dec;13(4):369-374. doi: 10.4103/ccd.ccd_782_21.
- Tent PA, Juncar RI, Onisor F, et al. The pathogenic microbial flora and its antibiotic susceptibility pattern in odontogenic infections. Drug Metab Rev. 2019 Aug;51(3):340-355. doi: 10.1080/03602532.2019.1602630.
- Bigus S, Russmüller G, Starzengruber P, et al. Antibiotic resistance of the bacterial spectrum of deep space head and neck infections in oral and maxillofacial surgery — a retrospective study. Clin Oral Investig. 2023 Aug;27(8):4687-4693. doi: 10.1007/s00784-023-05095-y.
- Kwon GB, Kim CH. Microbial isolates and antibiotic sensitivity in patients hospitalized with odontogenic infections at a tertiary center over 10 years. J Korean Assoc Oral Maxillofac Surg. 2023 Aug 31;49(4):198-207. doi: 10.5125/jkaoms.2023.49.4.198.
- Wang P, Huang Y, Long J. A Five-Year Retrospective Study of 746 Cases with Maxillofacial Space Infection in Western China. Infect Drug Resist. 2022 Aug 31;15:5099-5110. doi: 10.2147/IDR.S377657.
- Caruso SR, Yamaguchi E, Portnof JE. Update on Antimicrobial Therapy in Management of Acute Odontogenic Infection in Oral and Maxillofacial Surgery. Oral Maxillofac Surg Clin North Am. 2022 Feb;34(1):169-177. doi: 10.1016/j.coms.2021.08.005.
- Naim H, Rizvi M, Gupta R, et al. Drug resistance and molecular epidemiology of carbapenem resistant gram-negative bacilli isolates. J Glob Infect Dis. 2018;10:133-139. doi: 10.4103/jgid.jgid_74_17.
- Heim N., Jürgensen B., Kramer FJ. et al. Mapping the microbiological diversity of odontogenic abscess: are we using the right drugs? Clin Oral Invest. 2021;25:187-193. https://doi.org/10.1007/s00784-020-03350-0.
- Liau I, Han J, Bayetto K, et al. Antibiotic resistance in severe odontogenic infections of the South Australian population: a 9-year retrospective audit. Aust Dent J. 2018 Jun;63(2):187-192. doi: 10.1111/adj.12607.
- Yun JH, Kim SJ, Kim HS, Jung SY. Assessment of change in microbiology and antibiotic sensitivity of deep neck infection over 10 years. Korean J Otorhinolaryngol Head Neck Surg. 2021;64:327-35. https://doi.org/10.3342/kjorl-hns.2020.00157.
- Mungul S, Maharaj S. Microbiology of paediatric deep neck space infection. Int J Pediatr Otorhinolaryngol. 2019;123:116-22. doi: 10.1016/j.ijporl.2019.04.042.
- Salam MA, Al-Amin MY, Salam MT, Pawar JS, et al. Antimicrobial Resistance: A Growing Serious Threat for Global Public Health. Healthcare. 2023;11(13):1946. https://doi.org/10.3390/healthcare1113 1946.
- López-González E, Vitales-Noyola M, González-Amaro AM, et al. Aerobic and anaerobic microorganisms and antibiotic sensitivity of odontogenic maxillofacial infections. Odontology. 2019 Jul;107(3):409-417. doi: 10.1007/s10266-019-00414-w.